
Coronavirus
Well, it is all getting rather serious.
Please also monitor my Facebook page, as it is the most efficient way for me to disseminate information on a daily basis.
I will try to update every 1-2 days as time allows. I am also going to activate my Instagram.
For many doctors, our time has been crammed with taking in information from all the hospitals and health organisations, readjusting our private practices and caring for the people in front of us. So please be understanding if it is taking a bit longer to get back to you individually.
So,
I will see everyone tomorrow as scheduled, but after that I will most likely need to adapt to the requirements of the lockdown. It is likely that I will space out time frames between visits to reduce the need to travel outside your home.
The principles of care in the next few weeks are these:
• The less number of visits you need to attend will reduce risks to you, your baby, your partner, your family, me, my family and the greater community.
• The shorter the face to face interaction will also reduce the risk of transmission.
• The primary purpose of your visit is for me to physically examine you so that I have information regarding the size and position of your baby (and other things). I have done (literally) over 40,000 antenatal visits. I can get the information very quickly. All the time comes with explanations, reflections and discussion. This does not require a face-to-face visit.
• Don’t be offended if I shuffle you out the door. Everyone who knows me knows I like to chat. For all our sakes I need to curb that tendency. We can talk later.
• The longer I can avoid being exposed to the virus or contracting the virus the longer I can be available to deliver babies.
• The most important service I provide is to be available for deliveries. For ‘normal’ births, but more so for complicated births or caesarean sections.
• If I become unwell or am exposed, then you will be cared for by one of my usual roster of covering doctors.
• I will do my best to address your questions, concerns and provide a standard of care the same as if this bloody virus did not exist. I just need to be more creative about how that care is delivered.
• I will answer personal and individual questions privately but I will probably look to having a live ‘question and answer’ session over an hour every day or two. This might be useful to stay in touch and answer questions common to everyone. I will let you know about this as I work it out.
• Remember, still no kids or ‘extras’ at visits (partners ARE allowed – unless you want the peace and quiet). I want to thank ALL of you for respecting that so far.
My advice for consultations is this:
• If you have questions, have them pre-planned and ready to go. I will not be waiting while you contemplate the questions you have forgotten. I will answer your questions as I examine you and then you will be out the door (sorry….)
• If we have not covered your questions and issues, then you need to ‘register’ at the front desk as you leave that we did not cover everything you wanted and I will happily call you later that day (or next day if I run out of time). I will limit these phone calls to 10 minutes or so, as I anticipate making a lot of them.
• If I do call you later, I will try to do it during ‘business hours’ or late afternoon, but I may call you up until 10:30pm (I am a night owl). You may desire an earlier call, but I also have children who are scared and require my attention in the evening to maintain some normality in their lives. If you are in bed and do not answer that is fine, I will call the following day. If you haven’t heard from me by lunchtime the next day, then call the office (just in case I have overlooked your call for whatever reason).
• If I call I am likely to be a ‘no caller ID’. Don’t screen me out!
• The same rules (as outlined in your printed information) apply if you have a more urgent medical issue. Call the office during the day, call the delivery suite or if urgent then page me on 9387 1000.
• Last week I made a birth education video with our wonderful Fiona, an experienced midwife at St Vincents who runs the maternity education. It runs for 2 hours or so. (The blooper reel is longer….)
Over the next few weeks:
If I cannot be available (through quarantine, illness, whatever), then the other obstetricians in my covering arrangement will be available. They are also in the same situation. We have had discussions and meetings about helping each other out. More broadly, every obstetrician will be making themselves available for ANY pregnant woman in need. That means that if I, or any of my usual covering doctors, cannot attend a birth then it may be any accredited obstetrician at your booked hospital who may attend. They might be someone you have never met. They might be a man. They might be really young or really old. They might have bad breath. They might have a crap sense of humour. They will be qualified….and that might be the best we can do. Fortunately, all the doctors at St Vincents Private and Epworth Freemasons are fabulous. Of course, they are not me….but we are in desperate times. Good news is that I am FINE, unexposed, my family is well and I foresee that I should be able to keep working. I am just trying to reduce my exposure as much as possible for as long as possible.
A few things to consider:
It is completely normal to be overwhelmed, sad, scared, anxious, angry, feeling ripped-off.
Pregnancy is a particularly vulnerable time for most women. They are inevitably scared and anxious. They worry about their babies being ‘normal’. They worry for their own safety. They worry about pain. They feel disempowered about being so reliant on others to protect them. Or maybe that was just me…..
The good news is that:
PREGNANT WOMEN DO NOT SEEM ESPECIALLY VULNERABLE TO THIS VIRUS.
BABIES ARE NOT DEFORMED OR PARTICULARLY AFFECTED BY THIS VIRUS.
THANK GOD! (or whoever)
Remember that keeping fit is important – going for a long walk, being active and doing exercise will help you both mentally and physically.
Get off your phone – stop listening to all the depressing information. Read. Make plans. Do activities. Play games. Run around the back yard with the children (if you already have them). Make time to not engage with all the doom and gloom.
So, this will pass. We will come out the other side.
For women having their first babies, they will feel worried (over and above the usual worries) and feel ripped-off that their ‘self-indulgent’ pre-pregnancy time of spas and lunch-dates are not possible. Fair enough.
However, we live in a particularly lucky country at a lucky time in history.
This virus has shown how much we take for granted. Health, medical support, food, VACCINATIONS. (please slap the first anti-vaxxer you meet).
This is wartime. It is just that we face a biological enemy, not a human one.
So, we at least know the end will come, one way or another. It will diminish (like SARS) or we will get it and most of us will get better. Either way, IT WILL END.
IT WILL END.
Life will be different (although it is about time people worked out it is good to wash your bloody hands….!).
Remember, if you are feeling a bit precious about not seeing friends, not spending, not buying stuff….that most people in history have been through far worse. As those of you who are parents already know, and those of you about to have babies will come to understand…IT IS NOT ALL ABOUT THE INDIVIDUAL. As parents, we willingly make sacrifices for our child. Even if it hurts US.
There are times that you see or hear something that ‘smacks you in the face’ with its power.
For me, one of those time was watching a programme about the second world war. A Jewish woman recounted the last time she ever saw her mother. She was being shipped out of Europe by train with other children to be protected against the impending Nazi genocide. Her parents were sending her away to England, along with her older sister. Her sister was crying but complied with her parents demands to get on the train. The woman recalled how she clung to her mother and refused to get on. After much drama, her mother slapped her hard across the face. The young girl, having never been struck by her mother, was shocked and recoiled. She got on the train. She spent a long time upset with her mother’s harsh treatment and was angry and upset. Until later. When she realised that her mother slapped her on the face to stop her pleas to stay and comply with the demand to get on the train. Of course, in time, she realised that her loving mother took such harsh action because, above all, she wanted her daughter to be safe. She wanted her to get on that train, get out of Europe and survive. Tears sprang to my eyes. What shows the depth of a mother’s love more than a mother who is willing to be hated by her own child in order to make her comply with an order that will save her life. I often think of that mother. She must have collapsed with fear and grief and sadness to know her child was going to resent her for her ‘cruelty’ when she probably felt a visceral pain to let her go. I cried for hours.
So, this is not just about an individual. Whether you are already a parent or about to become one, we must all put aside our individual ‘rights’ and ‘desires’ to simply do the right thing. Follow directions. Respect the governments who are making the best decisions they can to keep us all safe. Remember that people have done it harder in the past. That this difficult time will come to an end. Lessons will be learned. Friends will be made. Priorities will be readdressed.
And won’t life be sweet on the other side……

Personal Protective Equipment
New PPE (personal protective equipment) in the office!
Hi dear patients and followers.
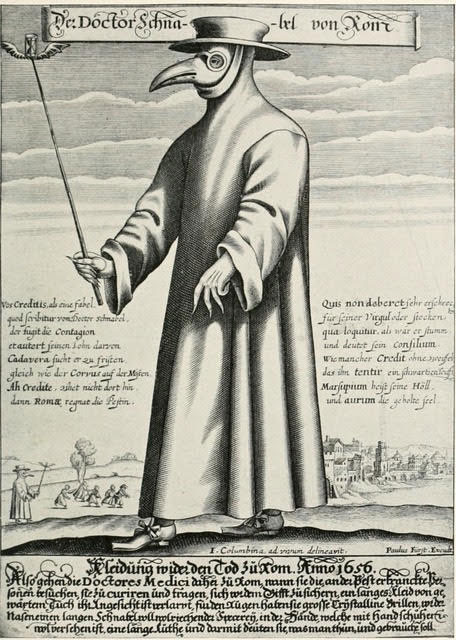
Just FYI, in keeping with the Coronavirus Carousel of Fun, I have arranged some new protective equipment for myself. Actually, it was my husband (as he loves me so much as doesn’t wish to see me infected with this new ‘Virus du Jour’) who has personally made and fitted my new ‘plague mask’. Yes, in accordance with my previously referred to ‘good old fashioned infection control’, I will be wearing a doctor’s plague suit into the office.
I attach photos of the originally documented medical plague doctor outfit, and photos of me suitably attired to attend to the patients. You will see why I have said no children in the office – might scare the bejesus out of them.
Amber
ps for those of you who are as gullible as I am it is only a joke. ha ha. I am completely hoping I will never need to go to such extremes. You can only imagine how terrifying it must have been in medieval times….
Medieval Times

Coronavirus Times!
How to keep your pregnant belly out of trouble (Pt 2)
To help stop everyone becoming Corona-Cray-Cray, I offer a small antidote:
Episode 2 of ‘How to keep your pregnant belly out of trouble’
#5 Wear dark clothes when you eat – or put on a serviette (Poirot-style) – unless you want to advertise what you ate for your last meal (when most of it ends up on the ‘belly-shelf’)
#6 Don’t stand too close to people in a queue. They can mistake your wriggling baby for you trying to feel them up. Both embarrassing and inappropriate coming from a pregnant woman.
#7 Be careful at kindergartens: pregnant bellies are just the right height for taking out a 4 year old. (Giving a pre-schooler a head injury is not a good look. The consequences could be dramatic enough to give Chris Tsiolkas the plot for the sequel to ‘The Slap’)
#8 Following on from #7, never arrive late at the theatre. The seats are so close together at The Princess Theatre that rushing along the row to get your seat for Harry Potter might cause a few Grannies to need craniotomies to fix the skull fractures and brain haemorrhages inflicted as your belly takes out their heads like a row of dominoes.
#9 Don’t try to hide behind trees with slim trunks
#10 Have baths not showers. Bellies are at exactly tap height in a shower. Those with modern taps are likely to bump them – next instant you are scalding hot or freezing cold.
#11 Don’t try to be the last one on a crowded tram or train. Squishing in at peak hour could result in an inadvertent caesarean section as the doors close.
#12 Don’t hug people who have recently had abdominal surgery
#13 Don’t go for the cheap Uber. It is embarrassing to send it away when you can’t fit into it. Even worse if it is Uber Pool. You would hear the others howl with laughter as they drive off without you.
#14 Don’t wear Spanx. Just don’t. You have no idea how ridiculous you already look and trying to force it into Spanx just makes you look like a fat gourmet sausage – and if someone gives you a poke your whole skin will split.*
#15 Don’t agree to wear a bridesmaid’s dress designed with as a short skirt with a small waist, full skirt and gold lurex material.**
Amber
*Thanks for the reminder Ali
** There are some things you cannot un-see. I still laugh out loud every time I think of the photo of my absolutely gorgeous young patient (including LOL as I write this!) more resembling Tweedle-dum.
*** The look of complete horror on her face was priceless.
*** Actually I think Katy Perry is trying to recreate the pregnant-Tweedle-dum look…but in pink.

May you live in interesting times…
“May you live in interesting times…”
We certainly do…
In response to the Coronavirus crisis, I am implementing some changes with regards to appointments. We need to take precautions to contain the spread of Coronavirus and I will be trying to do this. However, we must maintain our civility, keep our sense of humour and take appropriate and proportional steps.
I have sent an SMS to all my pregnant patients today:
“Due to Coronavirus, I am forced to implement the following: do not bring children or additional people (other than partner) to appt; do not attend if you have returned from overseas (anywhere) in last 2 wks; if you have fever, cough or are unwell you MUST CALL AHEAD for advice. I must protect pregnant women from exposure. Additionally, exposure of my staff may result in forced closure of the practice. If I am exposed or become unwell I will not be able to see patients or attend deliveries for 2+ weeks. Thank you for understanding. Further info will be on website and/or FB page.”
The community measures being taken to contain the spread of this virus seem extreme, but I am not an expert and I defer to more intelligent and experienced doctors and authorities who aim to protect our community. As with other viruses, the people most at risk are the immunocompromised – pregnant women, the very young, the elderly and those with chronic illness. As such, I need to take some action to protect my pregnant patients, in particular, and also my staff.
We have previously dealt with SARS, ‘swine flu’ and the common garden-variety Influenza. These have all represented a risk to pregnant women, with the benefit that at least there is a vaccination for Influenza that provides some measure of protection. Coronavirus seems more contagious, and it with this in mind that I am taking more precautions.
I recommend that only women (and their partners if necessary) attend for appointments. Children have no concept of avoiding coughing and sneezing over everything; slobbering, touching and licking everything in sight. People who are unwell clearly need to avoid exposing themselves to others (including my staff and myself). Although some countries represent a greater risk, there is no ‘safe’ country or ‘safe’ airport, so at this stage I recommend not coming for an appointment if you have come from overseas in the last 2 weeks. When in doubt, call ahead and we can make arrangements. I do not intend to avoid seeing sick patients – they need medical attention, of course – but calling ahead and giving us warning will allow me to take steps to appropriately protect my staff, other patients, and myself.
I recognise the difficulties in arranging childcare for an appointment. I will try to accommodate patients who need to reschedule due to lack of childcare. Likewise, I will accommodate patients who have come from overseas.
Just on Friday, a GP at The Toorak Clinic, a very good GP practice from which I get referrals, tested positive to Coronavirus. Despite having returned from the USA, not a country (yet ) deemed at risk, he has contracted the virus. This has forced the clinic to be closed. The ridiculous and offensive comments made by the Victorian Health Minister (who was ‘flabbergasted’ that a GP would turn up to work who was mildly unwell/ recovered and not returning from a high-risk country) indicates there will be no tolerance by the Government for healthcare workers, who have been exposed or unwell, seeing patients. Her comments indicate a complete ignorance of the way the healthcare system works (and she is the health minister…). Doctors frequently go to work and see patients when they are unwell themselves. So do other healthcare workers. If doctors stopped seeing patients when they had a sniffle, the whole healthcare system would grind to a halt. It is not that they wish to infect patients, but in my experience most doctors continue to work with disregard to their own wellbeing because, firstly, patients get annoyed if they are not seen as arranged (or are at risk because they cannot get medical care) and, secondly, they know the workload will fall to their colleagues (who are probably already overwhelmed with work).
As doctors, we consider the nature or seriousness of an illness (including how contagious it is), the risk to the patient, the special vulnerability of the patient and following the steps necessary to minimise the risk of transmitting a disease to our patients (or other staff). I have had THREE sick days in 25+ years of practice. This is likely due to being in generally good health*, practising extremely careful hand hygiene, being vaccinated, taking care to avoid contracting illnesses from my patients and sometimes pushing through despite my own discomfort. When I do push through and attend work I am meticulous to reduce risk to others.
The measures I am taking are simple. Less people in the office will reduce the risk of exposure. You will be asked to observe simple measures such as handwashing for 20-30 seconds before entering the office. Your child/ children or other people with you will be asked to wait outside. You may be asked to follow other directions. These precautions are all taken with a view to protecting everybody. This crisis is about more than the needs or desires of an individual patient. Please be respectful to my staff. They are at risk too. If we recommend rescheduling an appointment or decline to see you at a particular time, this is not a personal rebuke. It is simply old-fashioned infection control.
We must protect each other, and that includes my staff and myself. If my staff are infected, the office may be forced to close. If I am exposed (including if my staff get the virus) or I am infected, I will be forced to not see patients or attend deliveries for 2+ weeks. If my other obstetrician colleagues are similarly affected, any patient may be forced to see GPs or attend public hospitals (eek! ). In fact, for pregnant women, private obstetric care has the advantage of being booked in a hospital with an ICU* and seeing an individual doctor. It is easier to control the risk of exposure in a private setting than in a public hospital clinic.
Be reassured, I will never abandon my medical responsibilities. I have already contemplated, and am preparing for, the worst case scenario if I cannot physically see patients. This may include telephone/ video consultations and other measures. My primary responsibility will be to limit my exposure to avoid contracting Coronavirus so I can still attend and perform births. Of course, if I die from Coronavirus you will need to find another doctor (sorry….).***
I hope that everyone will be understanding of these measures. Hopefully, they may not be required for too long.
Amber
*Some would say it is only my sense of humour that is sick
**St Vincents Private has an intensive care unit. I hope you never see it…
***A joke but kind of true.

How to keep your pregnant belly out of trouble (Pt 1)
Driving home last night, a heavily pregnant woman and her partner stepped out from the parked cars to cross a busy road. Her pregnant belly grabbed my attention (her bright white A-line dress did nothing to hide it). I went through my automatic mental response: I wonder how many weeks she is? Is she my patient?? No! Why isn’t she coming to me? Oh, that’s right, there are a lot of pregnant women in Melbourne. Then I felt a bit protective and irritated. I wanted to wind down the window and yell: ‘don’t you know your belly is waaayyyy in front of you….Don’t stick it into the traffic! Be careful!!’ Then I checked myself; don’t boss around all the pregnant women! (Well, those of you I do boss around – you just keep doing like I tell you….!)
Then I thought: pregnant women need reminders about their pregnant bellies and how to keep them out of trouble. So I am starting a list:
#1 Don’t stick your belly into traffic (* couple of years ago I noted another woman who did this – except SHE WAS my patient so I chastised her at the next visit. I also tried unsuccessfully, in traffic, to pull over to offer her a lift)
#2 Remember when you iron your clothes that the iron is at belly height, so unless you want a permanent horizontal burn mark, be careful! (*I think women don’t iron as much as they used to – I used to see a lot more of these)
#3 wear clothes when you iron (see #2, at least only your clothes will get scorched).
#4 when you think ‘oh great! I nabbed that tight little car parking space!’ that you may not actually be able to EXIT the car like you used to (*message to my patient from a couple of weeks ago who clambered over her back seat and out the rear door because she wasn’t willing to find another park)
More to come (as I think of them).
More suggestions are welcome….
Spinal Muscular Atrophy Testing
This story is just tragic…and avoidable. Don’t worry my lovely patients, I have been doing all I can to prevent this happening to one of you. For years now, ever since the SMA test was available as a commercial test (no Medicare rebate), I have offered this test to every pregnant, post natal and would-be pregnant patients that I know may be considering a family in the future. If you have had the Cystic Fibrosis and Fragile X screening test then be reassured you have also had this test. Review the letter that I sent you with the CF and FXS results, it also contains the SMA screening results. I have had a handful of patients who are carriers but their partners were all clear. The test is available to anyone (public patients, private patients, anyone!), but unfortunately it is completely ‘out of pocket’ and the cost of $385 precludes many people from affording the test. However, often the issue is not the cost per se – some people will consider this test important and worth the money – but not even be aware that this test is even available. It can be ordered by any doctor. GPs and obstetricians all should have knowledge of this test. The beauty of this pre-pregnancy test is that if we find that both partners are carriers of SMA, then through IVF technology we can perform testing on embryos prior to transfer to the uterus so that women can be confident their babies are healthy. No doubt this innocent and unlucky couple will be doing IVF and PGD (pre-implantation diagnosis) in the future. It will never compensate them for the loss of their beloved baby.
Click here to view the full interactive story
Zika Virus
When you are pregnant, it is normal to feel paranoid about whether your baby will be healthy when it is born, and will your baby grow up to be a ‘normal’ child. The most recent reports about Zika virus will only act to send this anxiety through the roof. It is important that we look at the facts and make sure any precautions are taken to maximise the chance of a healthy baby in the event that you need to travel to an affected country or there is any spread to the Australian mainland (possible but unlikely in the foreseeable future).
Zika virus is a virus that is spread through mosquito bites. While it has been isolated from blood and semen, it seems that transmission is almost exclusively via mosquito bites. It is NOT spread from person to person through usual direct contact. As it is virtually always that infection is caused by mosquito bites, the main way to avoid infection is to avoid being bitten by mosquitoes. The mosquito that transmits the infection (the ‘vector’) is a particular kind of mosquito (aedes aegyptus) that exists only in TROPICAL areas. There is another species of mosquito (aedes albopictus) that lives in temperate areas which can also transmit the virus but this is less common. Hence, avoiding travel to areas where these mosquitoes thrive is recommended. Further, taking precautions to avoid mosquito bites also reduces the risk.

The most recent outbreak of Zika has been in Brazil. It has been noted that during the recent outbreak of Zika virus infection there has been a concomitant increase in the birth of babies with microcephaly. Microcephaly literally means small head. Many conditions can cause microcephaly, including other kinds of infections and specific developmental conditions. The concern with microcephaly is that it is usually associated with a smaller brain and related intellectual disability and developmental disorders.
While there is no doubt that Zika has been associated with increased risk of miscarriages and pregnancy loss, as well as microcephaly and intellectual disability, the exact way that it causes these serious problems is not completely understood. Further, how it affects development, and the impact of when during pregnancy is it contracted (ie how infection during each of the 3 trimesters), is also not completely understood. The most accurate thing that can be said is that the 20 fold increase in birth of babies with microcephaly in Brazil has occurred coincidentally with a large increase in the rate of Zika virus infection. Therefore, the logic is that the Zika virus is the likely cause.
Zika infection usually manifests in an illness about 2-12 days after being bitten by the infected mosquito. The illness caused includes fever (usually low grade: 37.8-38.5), rash, sore joints and conjunctivitis (at least 2 of these symptoms must be present to suggest the cause is possibly Zika virus). Other symptoms include headache, muscle pains and pain behind the eyes. Many infections can be ‘silent’ (or subclinical) whereby the infection can present without the patient being aware of having the infection. Even these ‘silent’ infections can be associated with a risk of having an affected baby. This is where the paranoia kicks in!!
Unless travel has occurred to an affected area, the likelihood is that there is another cause for the symptoms, including parvovirus, dengue fever, rubella, measles or other more uncommon infections. I routinely test all new pregnant patients for rubella and parvovirus, so I will be aware if you already have immunity to those particular viruses.
So what do I recommend:
1. Simply DO NOT GO to any countries where the offending mosquitoes thrives and/ or there is a current outbreak (check the CDC website (USA) or smarttraveller.gov.au. Sorry my lovely patients; NO trip to the Olympics! I don’t care what special corporate wiz-bang deal you may have been offered. Watch it at home!
2. Whilst the mosquito can live in temperate areas, there is currently no reason to believe the mosquitoes in Australia are affected. However, the virus has had outbreaks in Pacific Islands such as Samoa and the Cook Islands. It is possible that it could spread to temperate and tropical regions of Australia (FNQ, Northern territory, northern WA). I would possibly reconsider any trips to far north Queensland or pacific islands until we have a better grip on the situation.
3. It is sensible to be more strict about to covering up avoid insect bites. How do you do this:
- Wear long sleeves and long trousers.
- Apply insect repellent (DEET or picaridin containing). Forget the ‘natural’ repellants (citronella, eucalyptus, maleleuca, ultrasonic repellents). This is a situation where only tried and tested good ole chemicals will work.* The natural alternatives vary between useless (ultrasonic) to OK (oil of lemon eucalyptus) but only offer partial coverage and are simply not enough to protect you from Zika.
- Repellant can be applied directly to some skin surfaces but the best approach is to spray your CLOTHES and only apply repellent to EXPOSED skin surfaces. Do NOT apply repellent UNDER clothing.
- Purchase clothing/ bedding/ equipment pre-treated with permethrin or apply permethrin to these items.
- If overseas, use a mosquito net over the bed while sleeping.
*personally I feel the same when it comes to head lice treatment!! There are some things that require nothing less than chemical annhiliation….(just wait until your much loved little perfect baby turns into a mop-topped little toddler and comes home with a head full of lice. Trust me…)
With regards to insect repellent, it is appropriate to be cautious of pesticides. DEET, which is the main active ingredient in personal insect repellents, has NOT been shown to increase fetal abnormalities. When applied to skin it is absorbed into the circulation, thus a growing fetus is exposed to this pesticide. Therefore as explained above, it is more appropriate to apply DEET to clothes rather than skin. Another repellent is picaridin. It is a little stronger than DEET but does not last as long. Clothing and bedding itself can be treated with permethrin but it is not applied to skin.
It will be tempting to want testing to reassure yourself that you do not have Zika virus if you have travelled recently. This may be appropriate if you have been to one of the nominated countries that are affected, especially if you have had symptoms consistent with viral infection. At present the CDC in the US do not recommend testing for women with no symptoms and no evidence of fetal abnormality. This policy may change. The main basis of this policy is that the capacity for testing for this virus is currently very limited. We simply do not have the resources for a massive increase in testing, especially for the ‘worried well’ who have not even travelled to affected areas. Rest assured that this capacity is being reviewed and is likely to be ramped up in anticipation of an increased need to test women who have travelled to countries where Zika is already established or looks likely to be affected soon.
In the meantime I think the sensible approach is to avoid travel and step up your regime to avoid insect bites. (As you are probably aware I am not a great fan of women travelling during pregnancy anyway due to the unpredictable nature of pregnancy and the risks involved).
This infection is still being monitored and health agencies are active in trying to contain the spread and establish policies to protect pregnant women. In the meantime, watch this space!
Further information can be obtained from:
RANZCOG
https://www.ranzcog.edu.au/news/Zika-Virus
“There are concerns that pregnant women who become infected with Zika virus can transmit the disease to their unborn babies, with potentially serious consequences. The association between Zika virus and fetal malformations is still being investigated. However, rapidly accumulating evidence from the current outbreak appears to support a link between Zika virus infection and microcephaly and other serious brain abnormalities. Until more is known about Zika virus transmission in pregnancy and the association with adverse fetal outcomes, pregnant women should consider postponing travel to countries affected by the virus as authorities expand their list of places of concern.”
RANZCOG statement August 2016
RANZCOG Guidance
Care of women with cofirmed Zika virus infection during pregnancy in Australia (pdf)
The CDC website in the USA
http://www.cdc.gov/zika/geo/index.html
Smartraveller
http://smartraveller.gov.au/bulletins/zika_virus
WHO
http://www.who.int/mediacentre/factsheets/zika/en/
Australian Department of Health
http://www.health.gov.au/internet/main/publishing.nsf/Content/ohp-zika.htm
Countries affected by Zika:
I recommend that you appraise yourself of the most up to date list of countries through the Australian Department of Health website:
http://www.health.gov.au/internet/main/publishing.nsf/Content/ohp-zika-countries.htm
Insect repellants in Australia
- Aerogard – picaridin
- Bushman – DEET
- Off! – Picaridin
- Rid – DEET
Iodine in pregnancy and lactation
Iodine is a naturally occurring mineral that our bodies need for regulation of our metabolism. In pregnancy, the fetus relies on the mother to supply an adequate amount of iodine and, after birth, infants rely on breastmilk (or formula) to supply iodine.
The thyroid gland (a gland present in our necks; when it is enlarged it is called a ‘goitre’) requires iodine to produce thyroid hormone essential for regulation of metabolism. A deficiency of iodine or thyroid hormone in adults can result in fatigue, memory loss, dry hair and skin, slow reflexes and weight gain. In the developing fetus and in babies iodine deficiency can affect normal brain development resulting in lowered IQ, intellectual disability and diminished growth. Therefore, it is essential that pregnant and lactating women have an adequate daily intake of iodine.
So where do we get iodine from? Iodine content in food varies but is generally higher in seafood and dairy food, including eggs. A balanced diet will supply adequate iodine in most cases, but as pregnant and lactating women have a greater requirement, dietary sources may not be enough. Australia is now considered an iodine deficient country. This has occurred due to 2 main reasons: firstly, our increased consumption of processed foods has increased our salt intake but the food industry does not usually use iodised salt. Secondly, in the past, milk was stored in containers that were cleaned and sanitized using iodine containing disinfectants. The iodine in these cleaning agents leached into the milk. The iodine was theoretically a contaminant of the milk but actually was beneficial in supplying a significant amount of our daily iodine requirement. Now the dairy industry uses mainly chlorine based disinfectants so the iodine levels in milk have dropped.
How much do we need? Most adults require 150 mcg (MICROGRAMS) per day but pregnant women need 220-250mcg and lactating women need 270mcg per day. Fetuses will extract about 15mcg per day up to about 90mcg by term. Much of this transfer occurs in first trimester when maternal thyroid hormone production increases by about 50%. So as soon as a woman is pregnant her requirement for iodine increases significantly. Allowing an extra 100mcg daily from conception will cover this increased need.
Australia has a programme to assist people to get enough iodine into their diet. Bread is now fortified with iodine. This is mandatory. The only bread that escapes this law is ‘organic’ bread. This fortification programme alone increases the average daily intake by 50mcg daily. Also, salt is a major potential source of iodine. However, salt must be ‘iodised’. Natural sea salt does NOT contain much iodine. Therefore, using ‘iodised’ salt will add to our daily intake. Most Australian households have reduced the amount of salt used in cooking, but when they do it is often non-iodised salt. Simply replacing salt used in cooking or added at the table with iodised salt (it is on the salt packet – it has to be by law) will increase daily intake of iodine. Iodised salt contains approximately 200mcg per teaspoon (6g).
In addition, to ensuring adequate dietary intake (food or iodised salt) pregnant women may also need a supplement. Most multivitamins now contain iodine as an ingredient. It is usually recommended that a vitamin supplement contain between 150 to 250 mcg of iodine. There is no evidence that supplementation above 500mcg daily is beneficial. The maximum dose of additional supplementation is about 750mcg. Although only a small amount of iodine is stored in the thyroid gland and extra iodine is excreted by the kidneys, there is no safety data on taking more than 1000mcg daily so it is recommended to keep both dietary and supplement intake below 1000mcg daily.
Are there any circumstances where extra iodine supplementation should be avoided? Yes. In people with pre-existing thyroid disease having too much additional iodine may interfere with their thyroid function or medication requirements. Any iodine supplementation should only be taken under medical supervision. Also, some people are ‘iodine sensitive’.
What supplements can I take? As stated, most multivitamins contain iodine now. Check yours. Take into account the amount of iodine in the tablet and HOW MANY tablets you take daily. Additional supplementation can be taken in the form of iodine drops, iodine tablets (eg ‘Neurotabs’), tablet combinations (eg Blackmores I-Folic: iodine PLUS folic acid) etc. It is best to AVOID kelp supplements. Although kelp is a very good source of iodine (hence why sushi has a high iodine content because of the seaweed wrap), the amount of iodine in each kelp supplement can be variable AND the kelp supplement may contain higher doses of mercury.
How reliable is the test itself? The best test we have is a urinary iodine level. This measures the urinary excretion of iodine (hence a reflection on how much extra you have which is being excreted). If you are only excreting a small amount of iodine (less than 100mcg per litre of urine) this indicates that you are not getting enough iodine in your diet. Australian data indicates that the average urinary excretion of iodine in women is about 80mcg per litre and the average daily intake is about 130mcg per litre. This is well below the recommended intake. Ideally women should have a dietary intake of at least 220 mcg daily. Adequate dietary intake should result in urinary excretion levels above 100mcg and ideally above 150mcg per litre.
So what is my advice to you?
Be aware that I ROUTINELY test at 10 and 28 weeks. This is over and above the antenatal testing recommendation. I do so because my patients are extra special people who deserve extra intelligent children! My hope is they have all those extra IQ points to become doctors and don’t have to become lawyers (ha ha – sorry – no offence to all those lawyer patients of mine….)*
If I contact you after your 10 week bloods to advise additional iodine supplementation DON’T PANIC! You have not broken your baby! Tiny fetuses need very little iodine to begin with and will take what they need from you. If I advise a supplement I will PRESUME you are already on a multivitamin, so I will be recommending supplementation with an iodine supplement ON TOP OF the multivitamin.
If I contact you after your 28 week bloods to advise additional iodine supplementation DON’T PANIC! You have not broken your baby!!! If your initial result was normal and you are continuing to take your multivitamin then tweaking things at 30 weeks will just keep things well in normal range.
So:
- make sure your multivitamin contains some iodine.
- Make sure I am aware of which supplement you are taking (you should have noted this down at your first visit when you filled in the medical questionnaire).
- Make sure I am aware if you have specific dietary restrictions (eg if you don’t eat seafood or dairy) that may result in low dietary iodine intake (once again this information is requested on the questionnaire).
- If I advise extra iodine supplementation then take an extra supplement such as Blackmores I-folic 1 daily or Neurotabs 1 daily (others are OK – speak to your pharmacist). There is no need to contact me before your next appointment. I will discuss the result with you at your next appointment and if you are taking another type of supplement I will check this with you.
- See the foodstandards.gov.au website for a list of foods and their iodine content to help you determine any dietary changes you should make.
- Do not start taking excessive amounts of iodine. This may have detrimental effects on the fetal thyroid gland. Just add the supplement that I have advised.
- If you have an underlying thyroid condition speak to me about your individual situation.
*FYI my son is doing law this year at university…if only I had taken more iodine during his pregnancy ;-).
Coffee during pregnancy

OK. The coffee story: Overall it is agreed that moderate consumption of coffee is safe in pregnancy. So what is moderate and what can I drink you ask???
Caffeine is present in many beverage and food products, most commonly associated with coffee. There has often been a suggestion that caffeine is unhealthy in pregnancy. Caffeine does cross the placenta and is slowly metabolised by the fetus. In fact the fetus metabolises caffeine more slowly than adults and thus has a more prolonged exposure. Theoretically, caffeine can cause the release of a substance that closes blood vessels (‘vasoconstriction’) and therefore may be associated with reduced placental blood flow to the fetus. Also, some animal studies have suggested a link to birth defects in rats. This has not been seen in humans, although there are sources that say there is or may be a link.
The problem with studies in humans is there are many factors that make the study of caffeine intake difficult. Thus the data is inconclusive as many of the studies have inherent flaws. These flaws include: the link between drinking coffee and smoking (I know, I know – my patients don’t smoke – but studies of less well behaved people than my patients have difficulty separating the two habits and we KNOW smoking is bad for babies!); genetic variances between people (some people metabolise caffeine faster than others, therefore some fetuses metabolise the caffeine faster than others); the broad variation in actual caffeine content of various coffees and foods; the fact that most studies rely on patients to self-report their food and beverage (ie the pregnant person in the study tries to remember their caffeine intake – and we know how good a pregnant woman’s memory is!!); the blood concentration of caffeine is usually not accurately measured.
So taking all these factors into account it is very difficult to demonstrate with scientific certainty what caffeine does to the developing fetus. However, it is agreed between many learned organisations across Australia, the UK, Canada and the USA (amongst many other countries), that low to moderate caffeine consumption is NOT associated with birth defects. There is possibly a slight drop in birthweight of those babies born to mothers with moderate caffeine consumption but this appears to be an insignificant amount (about 50 to 70g).
There does NOT appear to be a link to miscarriage at moderate levels of caffeine consumption.
There does NOT appear to be any long-term harm from caffeine consumption.
There does NOT appear to be a link to premature birth.
So what is recommended as acceptable caffeine consumption? Most organisations agree that 200-300mg of caffeine daily is safe. What does this mean? Well an instant coffee is ABOUT 100mg (but who would want to drink that anyway?). Even decaf has some caffeine (about 5mg and ditto). A brewed or plunger style coffee is about 150-200mg and an expresso is about 200-300mg. Chocolate has about 5-10mg (a cup of chocolate). Tea has up to 50mg, green tea about 30mg. Soft drinks contain about 50mg per can but energy drinks are higher.
What do I think? Well I was caffeine free for my first baby (the peak of my good behaviour, just like most pregnant women with their first baby), my second I fell off the wagon – mugs and mugs of coffee daily (but he is a naughty little teenage liar now at the age of 13 – ???? – make your own associations!) and nos 3 and 4 I was BALANCED with a moderate approach (they are not liars). So I think it should be most wisely avoided in first trimester but a weak coffee is fine and for the desperate I think 1 expresso a day (or equivalent) is perfectly acceptable. For second and third trimesters I think 2 expressos daily is acceptable (a morning kick start and an afternoon booster) but if there are any other factors that may be affecting placental function probably best to avoid caffeine or just have a weak coffee.
Ironically, the studies suggest that moderate caffeine intake prior to conception seems to PROTECT against diabetes of pregnancy and caffeine intake during pregnancy PROTECTS again pre-eclampsia but…. I am skeptical so don’t use it as a justification for caffeine frenzy…..that can wait until AFTER the birth…along with the soft cheese and sushi frenzy…..
Morning Sickness: What Works?
Found an interesting and informative article regarding morning sickness on the abc website.
http://www.abc.net.au/health/features/stories/2014/06/25/4028941.htm