
Tips for Birth #1 – Labour
Understand and value the ‘latent’ phase of labour.
If we are to believe Hollywood (we don’t..) then labour takes about 6 minutes and birth about 2 minutes (it doesn’t..). I do not think that movies actually influence our perception of real life THAT much (seriously: Nicole Kidman aged 23 cast as a neurosurgeon. Really, Tom Cruise, we are gullible but not morons). However, there is a persisting belief that labour takes about 8 hours, ramps up really quickly and only starts when you don’t feel tired. Let’s have a bit of a reality check.
Often you hear women tell of their ‘3 day labour’ or ‘50 hour’ labour. They either tell you because 1. they wear it as a badge of honour (they endured so much..) or 2. they are horrified they were allow to labour for so long (surely the hospital is negligent..). In the eyes of maternity services providers, we know that most of that time is ‘latent phase’. Painful? Sure. Exhausting? Extremely. Traumatic? Often. Natural? Absolutely.
Here is what you need to know:
- Labour, especially the first one, takes a lot longer than you think.
- Women having their first labour and women having their subsequent labours are like 2 different species. Their labours are completely and utterly different. Latent phase is usually MUCH faster in subsequent labours.
- Labour does not always start and increase predictably; it can come and go.
- Labour can start just as your head hits the pillow and sometimes you will not sleep for 1, 2 or 3 nights in a row (apart from brief spells of 1-2 hours or lots of micro-sleeps).
I say all this not to frighten women. It is just the TRUTH*. Labour is a lottery. The best guide you have to predict your own labour is to know your own mother’s labour and birth history.
(*not just my version of the truth, Megs and Haz. THE truth.)
The hospital system does not support the natural progress of labour. Hospitals only want women to present when they are in ‘active’ labour. What does ‘active phase’ mean? You will learn in classes that there is a 1st, 2nd and 3rd stage of labour. The 1st stage is further broken down into the ‘latent’ phase and an ‘active’ phase of labour. The active phase is when the contractions are regular, predictable and moderately strong. It tends to progress in a linear fashion (the cervix dilates about 1.2cm per hour in first timers, 2cm per hour in following births). Labour is considered by medical staff to be active when the cervix has reached 4cm. However, that is all very mathematical. It can occur much more quickly, or more slowly, and can be linear or exponential in terms of the progress. Hospitals use a ‘partogram’ to depict this progress in a diagram. Whatevs. You can’t measure magic.
I think the problem is that we under-value the latent phase. The hospital system doesn’t provide time or space for women in latent phase.
Yet it is the most CRUCIAL phase (in my opinion).
What good is the latent phase?
- It ‘sets the scene’ for the progress in the active phase.
- It’s purpose of the latent phase is to slowly nudge the baby’s head into the pelvis.
- It helps the head rotate into the correct ‘anterior’ position: the position that is so crucial for the best fit into the pelvis.
- The slow increase in the frequency of the contractions (from every 10-15 mins to every 5 minutes) as well as the slow increase in the strength of the contractions allows a woman to ‘acclimatise’ to the labour. Humans are more likely to cope with pain when it builds up rather than being slammed with pain quickly.
The reason hospitals don’t support latent phase is that they provide staff according to ‘medical need’. Women in latent phase don’t have much medical need. They need rest, simple pain relief, reassurance. And time. Unlimited time.
Latent phase can take one hour or 40 hours. Contractions can come and build up. Or they last a few hours then stop. Then come back. This early ‘dance’ with labour is frustrating because women don’t know how long they will need to endure it. There is no ‘end in sight’. They worry because they don’t know if what is happening is ‘normal’. They look for reassurance. They ring the hospital. Multiple times. They are reassured that all is well but by the 3rd phone call they are invited in to be seen. They are tired and have had enough. If they are still only 1-2cm dilated on examination they are deflated and throw in the towel. They acquiesce to intervention- induction, epidurals. Now, BE CLEAR! I am NOT judging those women. I do not think induction or epidurals are bad. The desire to stay under supervision, to have stronger pain relief, to want things to move more quickly, to get some bloody sleep (!) are all completely understandable and appropriate. My issue is that women do not EXPECT latent phase to take a long time. They are not expecting or willing to be patient. They do not expect to be exhausted. They do not expect the extent of the pain that labour brings. They do not expect to have absolutely no idea that we cannot tell them how long it will take to get into ‘active’ labour. All we know is that it will eventually happen and to try to be patient until it gets established.
The absolutely brilliant thing that courses such as Calmbirth and Hypnobirth offers, is education about not being frightened of latent phase. To be patient. To be calm. To use alternative, non-medical means to cope with the long and frustrating and seemingly endless irregular contractions. They teach how to trust that your body is doing the right thing. It knows what it is doing. The use of terminology such as ‘surges’ rather than contractions is to help reduce the fear associated with the contractions = pain. ‘Natural birth’ courses teach patience and faith in your own body. That is gold. It is just qualified, by the fact that all the patience and faith in the world will not guarantee a ‘natural’ birth or a safe birth. It goes a LONG WAY, however.
Women are often reluctant to stay at home. What keeps them from staying at home?
Pain.
Sleep deprivation.
Fear.
How do medical people respond to those factors?
Give pain relief. Strong enough to allow sleep. Keep women in hospital help them feel safe.
The problem is that all these things can interfere with the ‘natural’ progress of the latent phase: the scene-setting phase.
You can’t put on a play or bake a cake or sit an exam or have a ‘natural’ labour without doing the preparation. Allowing latent phase to progress naturally will maximise the chance of the best positioning of the baby and the best conditioning of the cervix and uterus prior to the ‘main event’.
Now, of course, sometimes all the scene-setting in the world cannot guarantee an uncomplicated active phase or uncomplicated birth.
- There is no point staying at home if the baby’s health is compromised.
- There is no point in enduring latent phase if a woman is in agony, miserable or terrified.
- If latent phase is taking a long time, a check-up in hospital is appropriate.
- To be reassured that everything is normal.
- To check the baby is coping with the labour by doing a CTG (graphing the baby’s heart beat).
- To give some pain relief.
- To diagnose a problem or provide certainty or relief by way of induction or augmentation of labour to shorten the process.
- To arrange stronger analgesia such as epidural to allow relief of suffering and allow a woman to sleep.

So my tips are these:
- Have good quality antenatal care to ensure both mother and baby are in the best possible condition before labour even begins.
- Be mentally and physically prepared for the latent phase.
- Do not expect it to have a predictable time-frame. (Active phase is MUCH more predictable).
- Take simple pain relief (ie paracetamol) or have something stronger from your doctor (ie paracetamol with some codeine) to help ‘ease’ you into the discomfort of contractions and allow some rest between.
- By all means stay in touch with the birth-suite and report anything you are not sure about.
- Be prepared to come in for assessment and then,
- BE PREPARED TO GO HOME AGAIN. Sometimes the best thing you can do is have a check up for reassurance then go home again if the labour is not yet established. The actual dilation of the cervix is not as important as the nature of the contractions and the ‘descent’ of the head into the pelvis.
Personally, my philosophy is that women can give birth ANY WAY THEY WANT.
Your body.
Your choice.
Ideally, that means making a rational decision about both mode of birth and understanding the processes involved. That also means knowing the pros and cons of each.
It also means doing everything you can to minimise the risk of COMPLICATIONS that put mother and baby at risk.
If your plan is to have a VAGINAL birth, regardless of whether you are planning for ‘uber-natural’ or ‘elective epidural’ style birth, then embracing the latent phase will certainly reduce the risks of complications in labour and birth.
Often you read that having an epidural increases complications such as need for synthetic oxytocin drip or assisted birth. I do not believe that. It does, however, if you have the epidural TOO EARLY. By entering the active phase with a baby in the best possible position then even if you choose an epidural it will not slow your labour. Quite the opposite. It often speeds it up. The pelvic floor relaxes and, as the head is already in a good position, the fetal head can just ‘drop into place’ and descends into the pelvis perfectly with resulting rapid cervical dilatation. I believe it does not increase the risk of assisted birth providing a woman can have a bit of rest to re-charge, then have constructive guidance to push effectively and plenty of time to do so (up to 3 hours but usually baby is born within 1 hour of effective pushing).
So,
Have faith in your body.
Get some pain relief.
Get in the bath.
And be patient.
Should I have the Covid vaccine?
It’s new.
It seems rushed.
You are pregnant (or want to be).
Or you are breastfeeding.
You are nervous about whether to have it.
So here is my advice…
I cannot tell you whether you SHOULD have the vaccine.
I also cannot tell you WHICH vaccine you should have (presuming you even have a choice).
What I can tell you is what QUESTIONS you need to ask YOURSELF about the vaccine and about your own situation.
Then you can make a balanced decision about what to do in your own situation.
The Commonwealth Govt has quite a good guideline that I include a link to in the bio.
Questions you need to ask yourself:
Do I believe and trust the science?
The science behind vaccination is well established. Sure, this is a new virus. Sure, some of the vaccinations are based upon new approaches. However, none of the vaccinations include the ‘live virus’*, simply genetic replications of parts of the virus. It is not possible to ‘get’ COVID from the vaccination.There is no scientific reason to suspect that having the vaccination in pregnancy can cause harm to the developing fetus.
*some vaccines overseas are trialling a modified form of the live virus
How does the Immune System work?
You don’t need a year 9 science lesson but, frankly, if you want to make a considered decision then you need to understand the basics.
The three prongs of the system that protects us from infection are:
- The Innate immune system – an inborn system of immune responses we are born with. Cells recognise patterns for specific infectious particles. The capacity for infection recognition seems to be genetically transferred from parent to offspring. This system of protection against infection is, therefore, inborn and works immediately to protect the newborn before the longer timeframe required for the Cell-mediated and Antibody system to become effective. They are slower to get established but then become much more effective, fast and specific.
- The Cell-mediated immune system. Includes cells that search for infected cells and ‘T’ cells of different types. Cells in this system work together to kill virally infected cells and clear the infection and its aftermath. Proteins from potentially infected cells are presented to the T cells that kill the virus-infected cell. This system also supports the production of antibodies in the humoral system. However, whilst antibodies can PREVENT infection, the cell-mediated system is needed to fight and clear the infection.
- The Humoral (or Antibody producing) immune system. Antibodies are produced against invaders. These include different types of antibodies: IgG, IgA, IgM, IgE. Most importantly, memory antibody cells are created that remember specific invaders and rapidly mobilise to protect us when a second exposure to infection occurs. This is the basis of vaccination.
What are vaccinations? Are they all the same?
In essence, they all aim to trick the body’s immune system into recognising certain parts of a virus (in the case of coronavirus it is the funny little spikes on the surface of the virus – the ‘spike protein’) and provoke the immune system into making antibodies and other strategies to potentially destroy the invading virus. Most importantly, the immune system can respond very rapidly if ACTUAL infection with coronavirus occurs).
There are different vaccination platforms:
- Inactivate vaccines (Influenza and polio vaccines)
- Live attenuated vaccines (Measles)
- Protein or protein subunit vaccines (diphtheria, tetanus, Hep B)
- Recombinant protein vaccines (HPV vaccine – ‘Gardasil’)
- Vector vaccines (The Astra-Zeneca vaccine)
- DNA vaccines
- RNA vaccines (a completely new approach. Includes the Pfizer and Moderna vaccine)
The vaccines have been developed super-fast. Has there been enough testing?
We are so fortunate to have government agencies such as the Therapeutic Goods Authority (others include the FDA in the USA) that rigorously assess substances for their safety and efficacy before they are released for use in Australia. Being certain about a particular drug or vaccine takes time to evaluate. However, sometimes the threat posed by a communicable disease is so extreme that agencies must respond rapidly and take a balanced risk approach to authorising use of medications. Like Covid vaccines. However, this is a serious business and the TGA is very strict in Australia and does a thorough analysis of all the information. They carry the burden of making good decisions on our behalf. They do a good job.
How is the COVID vaccine tested for safety?
Essentially, getting new drugs or vaccines from concept to market involves 3 phases of pre-licencing testing:
Phase I assess safety, dosage and immune response in small numbers of people
Phase II larger numbers of people – hundreds – are enrolled to identify optimal dosing (how much, how often, how far apart)
Phase III thousands of people are enrolled to see how effective the vaccine is against the disease.
To get to the end of phase III usually takes about 10 years. The process has been truncated by overlapping the phases or combining them to save time but not compromise safety.
The crisis of coronavirus has compelled agencies to fast-track approval for testing and scientists are working double-speed to get results analysed and published.
Why aren’t pregnant women included in the vaccine trials?
They never are. There is a myriad of reasons why pregnant women are not put into trials, at least until a drug is already shown to be extremely safe in non-pregnant people or after following up pregnancies where a drug has been given ‘by accident’. The historical experience of drugs such as thalidomide has forever traumatised pregnant women, doctors, insurers and drug manufacturers. Nobody wants to take the risk that a new ‘trial’ drug might cause fetal abnormalities.
WE are fortunate that many pregnant women in the USA have been brave enough to have the vaccine, based on the theoretical safety of the vaccine based on the science. We are all waiting for the follow up information from studies of these women.
Is there a reason why I SHOULD NOT I get the vaccine?
Theoretically there is a RARE risk of a serious allergic reaction (as for ANY medication). This has been reported at about 5 reactions per 1 MILLION doses and usually in people with pre-existing allergic reactions. COVID-19 vaccines have not been ‘tested’ on pregnant women. It might not work anyway.
What side effects might I experience?
Soreness at the injection site
Lymph node enlargement
Fever
Tiredness
Headache
Muscle soreness
Fatigue
Am I in a risk group to contract COVID-19?
Yes, because you are a human being who lives in a community. As we all realise now, it can pop up anywhere, anytime, amongst anyone. Nobody is completely safe.
However, some groups are more likely to be exposed:
Healthcare workers, aged care workers
And some groups are more likely to get severe or fatal disease:
Elderly, people with pre-existing illnesses.
Should I just avoid COVID rather than get the vaccine?
Sure. This is the ideal situation. It is just not realistic.
Unless you plan to live alone in a remote cave, you will be potentially exposed.
Are you confident you will be one of the lucky people who gets no symptoms?
I would rather avoid this new vaccine (besides, I am not in at at-risk group) so do I really need it?
Are you confident that you will not unwittingly pass it on to your family members?
Are you confident that all the people you have contact with in your daily life will not get sick?
How will you feel if you pass it on to someone who gets sick or dies? How would you feel if that person was your partner, your child, your parents? Will you feel you did everything you could to protect them? Or will you rationalise the risk (they probably picked it up from someone else…)
Should I have the COVID vaccine if I am breastfeeding?
Yes is the short answer.
Breastmilk has loads of antibodies and other substances that support the newborn immune system. However, it is important to know that many of these antibodies are not actually available to the newborn.
Almost as soon as a human baby is born (other species are different), the gut closes to the absorption of IgG antibodies into the bloodstream. The main antibody that protects the newborn through breastmilk is IgA. This provides protection of the newborn’s mucosa (cells that line the gut and the respiratory system) against infection. It has been shown that breastfeeding protects newborns against gut infections (eg rotavirus, other diarrhoeal illnesses) and respiratory infections (pneumonia, RSV, COVID….(?) that attack across mucosal surfaces. However, newborns are not protected against all infections through breastmilk. Other factors in human milk support the newborn’s innate immune system. Antibodies are present but not all will be available to the newborn. Even if the mother is immune to diphtheria, for example, the antibodies in the mother’s blood will be excreted into breastmilk but they are not necessarily available to the newborn for its own protection (hence why vaccination is still critically important for babies whether they are breastfed or not).
Therefore, COVID vaccination will likely provide some factors that will help the breastfed newborn (and will not hurt the baby). However, the best protection for a baby is to have a mother that does NOT get the virus.
The vaccine might be SAFE but is it EFFECTIVE?
There are some differences in the effectiveness of the vaccines, based on information gleaned SO FAR from studies.
Pfizer – 95% effective after the second dose (a good vaccine but the need for extremely cold storage makes it difficult to deliver)
Moderna – 94% after second dose
Astra-Zeneca – 90% Some published data put this at a lower number – about 74% but further tweaking of the dose/ timing has improved the efficacy (this is currently the only vaccine that will be manufactured in Australia)
So in summary, I suggest you consider the following logical approach:
Am I a human being?
Yes (episodes of squealing like a pig when excited, working like a dog or screaming like a banshee does not diminish your humanity despite what your partner might say at times).
Do I live in a community?
Yes (Yes, you do, even if you hate and avoid your neighbours or annoying family*). *think Megs and Haz.
Am I wanting to get pregnant?
If yes, then have the vaccine as soon as you are eligible. (If you are an anti-vaxxer or a conspiracy theorist you have already made up your mind. You can discuss it with your own doctor but not me because I will be fully booked when you call for pregnancy care. I will be washing my hair that month and will only be available for existing patients and non-A-Vs). If you are open to vaccination but still have doubts, then wait a bit but be extra careful with the COVID avoidance principles.
Am I breastfeeding?
As above, I think yes – definitely get the vaccine.
Am I pregnant?
Your choice.
My advice is:
If in first trimester: then avoid until after 14 weeks UNLESS you are at high risk of ACTUALLY getting COVID. Given the low community transmission currently, it is reasonable to wait until after 14 weeks when most organogenesis (organ development) in your baby has been completed.
If beyond first trimester: your options are to avoid vaccination until after birth. I have seen stories on social media frightening women into not having the vaccination due to concerns about women not being included in the studies. However, as per my information above, the theoretical science and the experience to date would support the safety of the vaccine in pregnancy. FURTHER, as per the information above regarding breastfeeding, not all antibodies are available to newborns through breastmilk. HOWEVER, the mainstay for newborn protection against infection is the PASSIVE TRANSFER of antibodies – including IgG – ACROSS THE PLACENTA. These antibodies ARE available to newborn because the antibodies have already entered their bloodstream across the placenta. These antibodies will only last 2-4 months but will provide specific protection against infection until the newborn’s own immune system has had time to gear up. Hence, a pregnant woman who is vaccinated against COVID will create antibodies that will passively transfer to the fetus and still be available to the newborn baby. Many scientists believe this is will be the mainstay of newborn protection against COVID, at least as important, or even more so, that any breastfeeding protection.
Am I at higher than average risk of contracting COVID? If you are in an at-risk group, then being able to avoid contracting it may be difficult. Current levels of low transmission are not a guarantee the little blighter has gone away. If anything, the increasing vaccination rates are likely to lead to a much greater level of community complacency. Then we will see new outbreaks. Further, vaccination will allow more overseas travellers to return, bringing their pesky new COVID variants with them. As we know, our first line of defence (screening and hotel quarantine) is hardly watertight (and definitely not COVID-tight!).
Therefore, if you are at risk of COVID, cannot isolate, have other children (running around in the community and licking everything then bringing their germs home with them) or want to provide a higher level of protection to the newborn, it is reasonable to consider pregnancy vaccination. I admit that I, personally, would be vaccinated in pregnancy between 14-36 weeks (so the antibodies can form and cross the placenta), having now read the scientific papers. It is YOUR choice, however, and you should do what YOU feel most comfortable doing.
Of course I am willing to discuss your personal situation with you during a visit.
Update for Current Patients – 7th July (It’s baaa-aack!)
-Information
-Logistics
-Resources
-Advice (and ridiculous musings)
INFORMATION
It is annoying and worrying that we are once again in serious lockdown.
Things change daily so please keep up to date on Facebook and Instagram.
No excuses! We need you to stay alert and informed.
I am planning to do an Instagram ‘live’ tomorrow night at 18:00 hours. More details to come.
LOGISTICS
Here are the essential notifications:
I am away this week on ‘holiday’ (yeah…having a great time…sure am…carefree…party time!*)
Dr Suzana Kotevska is coving me this week and Dr Claire Francis will be on call from Friday night to Sunday night.
I will be back on call 20:00 Sunday night.
Despite having a fancy-free, exotic holiday* (*yes, sarcasm), I am monitoring the situation daily and will keep you as informed as possible.
Try not to call my office with procedural questions – watch FB and IG instead – but by all means call my office if you need to. I am in contact with the office daily (woo-hoo!)
For all of you that have an appointment next week I will be conducting telephone appointments WHEREVER POSSIBLE.
However, pregnancy care demands face-to-face appointments are still necessary.
You will be advised no later than THE DAY PRIOR whether I wish to see you in person or by telephone.
I will be making these recommendations on the basis of your individual situation. This takes into account your gestation and your personal medical situation.
If I have made a recommendation for Telehealth or face-to-face and you feel this is not appropriate for you, please just let us know. My recommendations are just that – a recommendation – but there are no hard rules. Let me know what you need.
Any face-to-face will be alone – no partner/ support person – unless you REALLY need your partner present. If this is the case you MUST let us know they will be coming with you.
If you live in a higher risk area/ postcode please let us know if you are coming in.
You MUST wear a mask at appointments and keep it on in the waiting room and during your appointment. I will be posting a video on how to wear a mask.
You MUST both wash your hands in the bathroom outside my office and ASLO apply hand sanitiser on arrival in the rooms BEFORE you take and don the mask.
Women in labour will STILL have a partner present (or support person if your partner is not well or not available). You partner may be required to wear a mask during the labour. Labouring women are not likely to be required to wear a mask unless they wish too.
Babies will NOT be separated from mothers.
Make sure you have a BP machine (see prior post)
RESOURCES
Keep up to date with the Victorian government website
https://www.dhhs.vic.gov.au/coronavirus
and the hospital websites
www.svphm.org.au
https://www.svphm.org.au/important-information-about-novel-coronavirus-covid-19
and
www.epworth.org.au
https://www.epworth.org.au/who-we-are/coronavirus-update
ADVICE
These rules are to protect YOU, your baby, my staff, hospital staff and me. We have families too.
The reason we are in this situation is due to people disregarding the guidelines and being complacent. (Grrr)
Trying to bend the rules because you feel like it (ie bringing in a partner who is not well) or being dishonest about your risk in order to get what YOU WANT puts others at risk – their life, their health, their families, their livelihoods.
I will always see women to care for them whether they have COVID or are at risk of COVID – it is my job, my vocation and my ethical responsibility.
However, knowing if there is a risk means I can wear appropriate PPE (personal protective equipment) to reduce my risk of contracting COVID-19.
You may not be aware that I am personally on medication that suppresses my immune system such that I am more at risk of serious disease or death if I am infected (then I will never see who wins Big Brother!).
Being honest and upfront about your situation allows me to protect myself and my staff and other women and their babies. So please let us know if you are potentially at risk.
This is a really, really, really difficult time for everyone and to be pregnant and a new mum at this time is the pits.
So keep communicating with us! Be confident I will be staying COVID-free to make sure I remain THERE FOR YOU!
Keep things in perspective.
Keep your sense of humour – hence I will post a stupid video on stretcher epic-fails that is possibly more dangerous than COVID ( I nearly swallowed my own tongue from laughing so much….)
Update for Current Patients – 7th April
A quick update and an apology
1. The office is closed today
Leave admin stuff until tomorrow. We will be there bright and early Wednesday morning. More urgent medical issues follow your usual procedure as you would if it were a weekend. I am still available today but working from home. If you want a home birth you will have to come over to my place.
2. An apology
I have activated my Instagram account (come follow me!!! I need to break the internet!). I posted a mini version of the BP measurement video. However, it has brought to my attention that it was somewhat disconcerting and disappointing to the viewers that it was NOT funny. For that I am UNASHAMEDLY sorry.
For those of you who have been under my care you know that I can be serious when I need to be, but otherwise most of my day I can’t help seeing the funny side of things. Patients are an endless source of fascination to me and there are so many things that make me laugh. They make me laugh. I make them laugh. We laugh at their partners – usually when they are present (makes me feel better about the dumb things my own husband does). Then, without warning, I had the audacity to post MEDICAL instruction video WITHOUT being FUNNY.
Please forgive me, it was my first video and I am learning. I have opened a YouTube account…..and now TikTok. Maybe I can use those media to satisfy my patients’ needs for amusement! I will do whatever it takes to look after you ladies! I started to check out if TikTok was appropriate to use but got stuck on #ifhumansactedlikedogs. Hilarious! Maybe we can get all of you to post funny little pregnancy videos for my account (not like the Amy Schumer one – we could do better). I promise it won’t be like DrPimplePopper. More like DrBabyPopper.
I am sorry for my lack of mirth. I will try not to do it again.
So….

Don’t Panic the Baby is Safe!
Women who are feeling despondent about IVF and other assisted reproductive techniques being side-lined need special support at this time. I want them to know that their ‘test-tube’ babies are growing and ready for them to collect in 2021!
The baby shown is actually in a medical device (called a Pigg-o-stat) designed for infants – two year olds to hold them still while they are being X-rayed. I don’t think they are used in Australia (bit disappointing really… I would love to have a photo of one of my four in the Pigg-o-stat).
Actually, I have posted a video on ‘the gram’ (see how cool I am Sarah Rowley) about Volde-virus and whether to have a baby or not, as well as concerns about IVF services. It is only short and doesn’t cover everything (obviously) but I will write more about it later.
In the meantime, follow my INSTAGRAM account to see more of these cute chubby little baby photos. Adorable! (but kind of unsettling. They look more confused than distressed) Don’t even google them – there is a dark side to people’s response. I just think they are super cute.
I don’t care about Coronavirus! I want a baby!!
Check out the video regarding whether you should try for a baby and what about IVF and reproductive technology?
Update for Current Patients – 2nd April
-Logistics
-Information
-Resources
-Advice (and ridiculous musings)
LOGISTICS
Visits continue as planned at present but next week I will likely recommend more telephone consultations. I will contact you if I recommend this in your case, or you may call the office and request a telephone consultation if you prefer.
Remember that you will be screened upon entering the hospital.
Please do not bring your partner or anyone else unless you feel your partner’s attendance is necessary. If you do, then I have no problem with that provided they are well (remember if they are not they may be prevented from entering the hospital).
Caesarean sections and inductions of labour are unaffected by the C19 situation.
I will still be recommending waiting in your car in between GTT blood tests, but if you are not well this may not be a good idea. Sometimes the GTT causes women to feel nauseous or faint. That is why I usually recommend it be done at St Vincents on a day you are seeing me. If you are unwell we will care for you.
Traffic is great but parking still a bit tight. Those people going to work are preferring to drive than use public transport so the car parks are still full. I think St Vincent PUBLIC has closed their carpark to visitors (staff only). St Vincents Private car park is still available and so is still busy.
Remember to try to obtain a blood pressure cuff. If you have obtained Uristix that is great. If you have not then we will give you some at the next visit. Take a photo of the legend on the container (and I don’t mean Gary Ablett, I mean the colour labels to tell you how to interpret the result).
INFORMATION
I have been unusually busy with actual births, consultations, questions and admin in the last 2 weeks. I have checked all results coming through and received lots of questions. I did not even go home overnight of for 2 nights in the last 2 weeks. Not to mention my sore knee….. (poor me…sob)…so I am a bit behind in chasing up details and making phone calls. I have making my way through all of this. Sorry, not superhuman. I often check through things and make sure there are no serious concerns but then need time to address things in detail. This takes time and I would rather do it carefully and methodically. Sometimes I wonder how my colleagues seem to leave their offices so early. Don’t they have paperwork to do?????
Anyway, I am catching up. So if I have something I need to do for you or you are expecting a call, please know that I make take time to do things, but I never forget. If you have a concern, please just call the office to let us know. I am sorry I did not report last night that the office was closed today but the information was on the answering machine message. It will be more common that the office will be closed once per week.
Urgent calls can still be directed to the birth suite if you are over 20 weeks gestation and/ or you can page me on 9387 1000 if you are under 20 weeks or have a matter to wish to speak to me about directly. Where possible, please leave the paging service calls for urgent medical matters. Non-urgent calls can be made to the office during business hours. Administrative matters – appointments, referrals, certificates, other paperwork etc should be directed to my staff, Erin and Zoe, during business hours.
RESOURCES
Couple of resources to remember just FYI:
A great resource for women with diabetes in pregnancy. There is a very good ‘FAQ’ section.
General patient information brochures – obstetric and gynaecological.
There are lots of pregnancy related information pamphlets on this link. Check your USB card – I have downloaded many of them for you.
https://ranzcog.edu.au/womens-health/patient-information-guides/patient-information-pamphlets
ADVICE (and ridiculous musings)
I see that the doctors who apparently ‘absquatulated’ (see previous post) when told to self-isolate claim they were instructed they could leave for domestic flights. Upon reflection, I think it would be very unusual for that many doctors to disregard explicit instructions (there is always a few but 27 out of 33??). One of the doctors who remained at the airport I have worked with previously and he is an honourable man and excellent doctor, Professor Shane Hamblin. He supports their claims that the group were told they were allowed to leave. If he says that, I believe him. My statement remains, however, if doctors disregard instructions, how can we expect anyone else to do so.
———————————–
You may see that I have been busy in the last couple of weeks recording childbirth education classes for the hospital. Some of you will have been sent the link and, hopefully, have seen them. On Tuesday night I participated in a live stream to the antenatal childbirth class patients with Fiona Hamilton. Fiona and I are getting the hang of it a bit more now and we are planning a career in television…goodbye obstetrics!!!! Only joking! I will be delivering babies until my knobbled arthritic fingers are too crooked to fit into the birth canal (!). Unless I get lots of patients with abnormally shaped birth canals….* Fiona and I have been rather stressed but had lots of fun. It is SUCH a joy to share an experience with a long-standing colleague. Fiona worked in the birth suite for many years and was a gifted midwife. It has been such a loss to women that she is no longer actively doing deliveries. She is, however, now making a much greater contribution to even more women in the important field of childbirth education. She is calm, experienced, informed, caring, intelligent and bloody funny. Working to make the videos was a joy for me and I hope the respect that Fiona and I have for each other and our respective fields comes across in the videos.** We are all after the same thing and it is really simple. Healthy mum. Healthy baby. Caring for women in pregnancy and childbirth has been a rather political issue at times. As a feminist, I have often felt the pull between promoting and empowering women to birth naturally and without intervention. As an obstetrician, I feel the overwhelming need to inform women of risks and protect them from the harm that can come from the natural process if complications occur and medical care is not provided. Over the years, this push and pull (no pun intended…) has relaxed and I now simply support the choice of women to give birth whichever way they want. No pain relief, minimal intervention, elective analgesia, home birth, elective caesarean section. Whatever. Being a grown-up also means taking some responsibility for your own health, so whichever path is chosen, it is crucial that women ask questions and arm themselves with information. They must also be flexible to adapt to a changing circumstance that might require a deviation from the plan. Planned low intervention vaginal births sometimes require intervention, women choosing elective caesarean section sometimes go into labour. Be informed. Be determined. Be flexible. Take advice.
*My husband thinks it is better for everybody if I just keep working until I drop. He thinks I am dangerous when I don’t have enough to do. He is probably correct. OK. He is correct. (However, clearly a TV career could change things…). The only likelihood of me retiring is if I win Tattslotto. Then his opinion won’t matter. The tickets are registered in my name and he will have to work out where I have gone first…
**If I look like I am looking at her intently during the videos and on the verge of laughing it will be because we were in hysterics off-camera just before that segment.
———————————–
Excitingly, I have activated my Instagram account. It is fledgling and this old bird is just working out how to use it. Even did my first ‘tag’. So be patient with me if I muck it up. It will be largely for fun and a complete waste of your time (let alone mine… Sonya, look away….it is just another social media drug). I am fascinated to see what my colleagues are posting. Some are great, some are completely mind-numbing, some are completely self-indulgent. Of course, mine will be probably also be self-indulgent but more likely just silly and immature (sorry guys, that is me. Still laugh at poo jokes. A university education does not make you immune to that).
I love love love newborns and infants, however, I will not be posting photos and details as some of my colleagues do. Frankly, I have a bit of an issue with the exposure of a child and family’s privacy. Publishing the date of birth, gender, parents names etc is not wise in my opinion. Certainly not for a doctor. What parents choose to do is their business. I will not, however, expose a patient’s or baby’s details for the purpose of self-promotion. It is not difficult for someone with evil intentions to obtain a lot of personal information with a view to identity theft or some other nefarious purpose. I know that my colleagues certainly mean no harm and they are celebrating with the family. However, I also do not want my patients to feel pressured to have a photo taken with me for my benefit. So I will not be doing that. If you want to have a photo with me I will be delighted but I will not publish it myself (you can). That is your business. I may ask to have a photo of your baby with me. I am happy to publish that on FB or Intragram, but ONLY if you request it or freely agree. I figure that babies change so rapidly that an unidentified photo of them cannot be used for evil purposes. Hence, my many silly obstetrician-baby selfies. I may put them on Instagram. If you have the slightest issue I will not post it. No questions asked. If you WANT me to post a super-cute photo of your baby (ideally with me in it for the purposes of my account but not necessarily with me. It might be with someone else). I have an enormous library of cute babies and quirky work photos from over the years. Send me one if you want to see in on Instagram!
———————————–
A big thank-you to my patient’s partner (you know who you are..), who recently told me a story (after the birth of the baby) about one of his own medical experiences. I have been chuckling to myself all day and couldn’t stop laughing when I was trying to tell my husband. I will never hear the word ‘uvula’ without thinking of you and laughing. (it is a pretty silly word anyway).
———————————–
Re volde-virus (AKA C19):
I attach a photo of the face mask my husband had delivered the other day. He opened one of the several packages that had been delivered. He put it on. I looked on curiously. “Did you buy that for me to use at work to protect me from volde-virus?” I was both impressed at his forward planning and endeared by his concern to protect me and our family. “No”, he said matter-of-factly, “it is a snorkel mask with an inbuilt mouth piece. I have been trying to clean the pool filter and need to be underwater to do it properly. This means I can see and breathe easily while I am doing it. Cool huh!?!”***
***apparently since then there are surgeons who are looking at adapting these kinds of masks against C19. Maybe hubby is ahead of his time.
Update for Current Patients – 29th March
-Logistics
-Information
-Resources
-Advice (and ridiculous musings)
LOGISTICS
Presently appointments will continue as scheduled. However, I need to keep them brief and I will likely get stricter on this. It will be light super-high-speed-patient-doctor dating. (If we ‘click’ I’ll get your number and call you later…..just joking, I’ll call later if we need to talk in more detail or you don’t get all your questions answered).
Have those questions ready to go. I can examine and talk at the same time (not like the male doctors; I can multi-task 😉
Maintain social distancing in the waiting room (see the photo from the other day)
You don’t need to wear a mask to your appointment but you can if you feel more secure. At this stage I will not be wearing a mask.
You will be screened on the way in to the hospital – questioned, temp taken. Non-patients may be excluded. Anyone with temp might be excluded. If you are a patient you may be stopped from coming in until I have been contacted.
Please don’t even try to come in if you are unwell. Call ahead. We will deal with it.
The new change I am implementing is to encourage you to COME ALONE. I understand that you might prefer your partner to be with you. Sorry. You know that I like to make fun of male partners in particular (albeit in a caring way….)
However, I understand that some women they have an important reason to have their partners present. The greater need for your partner may also apply if you are in late pregnancy / have concerns about the welfare of the pregnancy or woman / need to touch base about delivery etc. My own opinion is that pregnant women come as a ‘team’ with their partner (male or female), so although the woman herself is ‘the boss’ and theoretically my only ‘patient’, caring for women means caring for the family.
So ALL I ASK is that you don’t bring your partner unless you have a genuine need or strong desire to have your partner present. If you feel that way, then I have no problem with you having your partner present (I figure you are both so exposed to each other it is probably illogical to consider they might be positive but you are not. However, look at Charles and Camilla…. Try to figure that one out after ‘tampon-gate’)
Don’t forget that I am willing to call you later and speaker-phone allows us to have a discussion with your partner (and anyone else present – you mum, whatever) present and involved.
Although I am willing to see you if you are well, I will be reviewing the patients due for the following day and might determine I would prefer it to be tele-health. I will contact you if I recommend this. If you do not hear from me then attend as scheduled.
Importantly, if YOU would PREFER a tele-health call rather than face-to-face then simply call the office and request it. I will try to call you during the allocated appointment time but it may not be possible. I will get to you. I will usually SMS ahead of the call to give you warning.
INFORMATION
The RCOG has updated their information regarding Volde-virus and pregnancy.
Statement from the British (Royal College of Obstetricians and Gynaecologists) O&G website (they have been very up to date and informative):
Vale
Last week, we lost a true saint. Catherine Hamlin. If you have not heard of her, google her. She was born into a privileged Sydney family. She qualified as an obstetrician/ gynaecologist in the 50’s. She, and her Ob/Gyn husband, Reg Hamlin, travelled early in their careers to Addis Ababa, Ethiopia. They established the Fistula Hospital. Why? Because they witnessed and treated the mass of women who suffered unbelievable injury directly resulting from childbirth. Long labours, malpresentations of babies, non-existent obstetric care and only rudimentary midwifery care led to pelvic injury of the type Western women cannot even imagine. She treated HUNDREDS/ THOUSANDS of women who arrived in rags. At a young age they had been in labour for DAYS AND DAYS. Their babies were dead inside them. The birth process to deliver their dead baby had resulted in permanent injury to their pelvic organs leading to chronic loss of urine AND/ or faeces through their vagina. Can you imagine it???? The reaction of their husbands and families? Not to help them. No. To shun them. Cast them into the streets. They died, became beggars. All of this while grieving the loss of their babies. As news of the establishment of the Hamlin hospital spread, women walked hundreds of miles to seek the life-changing surgery. To make them continent. A simple desire. She remained in Ethiopia until her death last week aged 96. She continued to operate but, most importantly, she trained doctors and passed on her skills so the care continued beyond her lifetime. Very few people or doctors leave the kind of life-changing legacy that she did. I am humbled by her gift to humanity. I feel inadequate and privileged in the face of her commitment. I can only aspire to make any sort of positive change in peoples’ lives that is a fraction of what she achieved. I had the honour of meeting her years ago when she launched her book ‘The Hospital by the River’ and she signed my copy. Get it. Read it. AFTER YOU HAVE GIVEN BIRTH!!!! (for God’s sake…there is already enough to feel overwhelmingly anxious about without reading it at the moment). However, it is important to realise that women throughout the world are incredibly traumatised by childbirth. Still now, the Mercy Ships that dock in 3rd world countries to provide surgery and treatment encounter queues that are MILES long of women with the same problem. A problem we rarely see here (or at least to the same degree) due to good midwifery and obstetric care. Yes, C19 is currently proving how lucky WE are.
Vale Catherine Hamlin.

Dr. Catherine Hamlin

Dr. Catherine Hamlin at the Hamlin Fistula Hospital, Ethiopia
RESOURCES
It is all quite overwhelming so I repost the link for dealing with the anxiety created over VV (volde-virus)
https://headtohealth.gov.au/covid-19-support/covid-19
(if these updates are causing the same effect then stop reading them. Just skip over the above and go directly to musings).
ADVICE (and ridiculous musings)
Highlight Of The Week: delivering a baby named AMBER!!! Yay!! Obviously, she was really cute and had an uncommonly intelligent look on her face.
Lowlight Of The Week: Kenny Rogers died. Singing ‘Islands in the Stream’ with my friend, Andrew White, will be so much more melancholy after this is over and karaoke gets back to normal. Kenny really understood when it was time to ‘know when to fold’em’.
Increasing The Community Vocabulary #1: I am so excited to see the phrase ‘don and doff’ come back!! Yes, we ‘healthcare workers’ are watching videos on safe ways to put on (‘don’) and take off (‘doff’) our PPE (personal protecting equipment). Love the word ‘doff’. Might start using it in real life. “Patient, I need to examine you, please doff your underwear”. “I think your newborn’s nappy is full. Please doff the nappy”. “Nurse, I cannot get my surgical gown off, please help me doff it”. Awesome.
Increasing The Community Vocabulary #2: my new favourite word (courtesy of a teenaged son) ABSQUATULATE. Means to leave abruptly. I am reserving it for a special occasion. Like when I am in the middle of a vaginal examination and the patient tells me “By the way, Dr Amber, I have coronavirus (or could be anything else – Ebola/ smallpox/ SARS)”. Amber (withdrawing fingers). “Sorry patient, excuse me, I have to absquatulate”.
Finally, a rant (apologies if you disagree, we are all entitled to our opinions).
I think that when this is over, people will naturally go back to their old ways. It is human nature. It is this ability to just keep going and ‘forget’ that is our greatest strength. Otherwise why would women have a second baby????
I can only hope that after this whole debacle we will get some permanent changes in this country:
I hope that as a country we become more self-sufficient.
I hope that we realise how important it is that we maintain manufacturing. We need to be able to manufacture sophisticated medical equipment. Parts for important machines (like for one of our lifts that has not been working for weeks awaiting parts from ‘overseas’). Packaging. Medicinal drugs.
I hope we realise that there is a balance between paying a low price at the checkout versus keeping jobs in Australia. I am always prepared to pay more for Australian produced items that employ Aussies. Just recently I was at a conference talking to a rep for a drug product I regularly prescribed. She was spruiking her brand (Oripro). She made one statement: ‘it is manufactured in Australia by an Australian company.’ She kept talking. I stopped her. “you had me at made in Australia”. I have prescribed this exclusively since.
I hope that the consumer stripping (almost conspiratorial theft!) of items such as baby formula, Elevit, Blackmore’s Pregnancy Gold etc, medical equipment to be sent and sold overseas is outlawed and stopped in the stores. I make no comment on the countries involved or the likely reasonable rationale for those people to do it, but it is simply unfair to cause our citizens to be anxious about getting something as vital as baby formula. It underscores the fact that other countries recognise the high standards of the items we do produce. If our products are so good, then create a legitimate export market and jail people who strip our shelves and place us at risk of social unrest as a result.
I hope that people truly value our healthcare system. THE BEST IN THE WORLD (or really close). As many of you are aware, I have done a law degree and, more recently, a masters of law. One of my subjects was ‘comparative health law’. Our system is amongst the best in the world for outcomes….and ‘mid-priced’. It is comparable to the UK. America is a joke. Most expensive by far and worst outcomes. The point is, we are ALL entitled to Medicare. Free hospital care. General practitioner services were NEVER SUPPOSED TO BE FREE. They were meant to be heavily subsidised so they were affordable. A few unscrupulous doctors* and entrepreneurs opened ‘bulk-billing’ clinics with the business mode of reduced price (free at point of ‘purchase’) to enable direct payment from government (so not relying on patients to pay the bill). The whole reaction against a co-payment is rubbish. Just a political thing. If the government had allowed ‘co-payments’ when the bulk-billing guys (and they were guys) were setting up, we would be in a completely different situation. We have a fabulous, not perfect, system. Public hospitals are generally excellent. Private hospitals are generally excellent. We have a specialist medical workforce that feels obliged to work in, and give back to, the public system even if they have successful private practices. Australians are privileged to be able to purchase private health insurance (not just related to their employment as in the USA) and exercise their choice to go private or public according to their needs and finances (not like the UK). I know private health insurance is expensive. I pay it. However, our system is the best in an imperfect world.
Value it.
I hope that our hospitals will continue to be cleaned as much as they are now. Let me tell you that EVERY hospital in Australia has dropped their standards over the years (except for the operating theatres). Visitors and kids running amok. People everywhere. Cleaning budgets reduced. Hospitals have a reason to be worried about coronavirus spreading. For the first time last week I entered a ward that SMELLED LIKE IT WAS CLEAN. I had not experienced that since I was a child.
I hope that hospitals get rid of carpets and put in linoleum that is cleaned properly and frequently.
Finally,
BE CAREFUL WHAT YOU TELL YOUR CHILDREN!
Heard one of them sneeze today.
I called out “I heard a sneeze, STERILISE YOURSELF”.
JUST got to him before he cut his testicles off.
“No, idiot, I mean DISINFECT YOURSELF”.
Phew.
Stay well people.
Stay in touch.
For those of you who have received the link to the online video for the classes, don’t forget to tune into the live feed on Tuesday night. Be kind. I’m nervous. The other doctors’ patients might be mean to me.
xxx

Update for Current Patients – 25th March (Evening Edition)
Good evening lovely patients.
– Logistics
– Information
– Resources
– Advice (and general ridiculous musings by myself to you)
LOGISTICS
- Office open tomorrow from 8am.
- Staff will arrive 8:30 so phone calls after 9 please.
- Still only partners, no kids, no others (unless previously arranged for very specific reasons. *No Jessica, you can’t bring Meghan Markle. I don’t care how much she wants to spread love and improve our mental health).
- Visits will be brief. Have your questions ready. Register at the desk on the way out for a call later if you need one.
- Please bring your OWN PEN to sign documents. You cannot use mine and it is too for me to clean a pen after every use.
- If you have purchased a BP machine (as I have previously requested by SMS – yay for you if you have) then take BP in the morning before you leave home and write it down so you are ready to tell me the result. I may take your BP myself anyway but please get into the habit).
- If you have purchased Uristix, have a go at peeing on the stick and interpreting the result. DO NOT STRESS if you have not bought the BP machine or Uristix (some people are reporting they have been unable to buy them). I will talk to you about it. I am hoping that patients may be able to on-sell a BP machine to another patient of mine down the track to recoup some of their outlay.
- If you are scheduled for a Glucose Tolerance Test (GTT) in the next couple of weeks, I suggest you start at 9am as indicated in my information sheet. Park in the car park behind St Vincents Private. In between blood tests at 1 and 2 hours go back and wait in your car. (Tell path you are doing this or just lie to them and come directly up to me. Sorry, not ‘lie’, that would be bad. Just be ‘vague’.) Regardless of your ‘true’ appointment time, come up after one of the blood tests and I will see you next. As the visits are brief these days anyway (it’s killing me…can’t have a laugh…can’t tell an anecdote…I am becoming addicted to social media, good grief!) you should not have to wait long.
INFORMATION
The most important information regarding pregnant women and C19 (volde-virus) is contained within the RANZCOG (our obstetric college) statement:
https://ranzcog.edu.au/statements-guidelines/covid-19-statement
“However, at this time, pregnant women do not appear to be more severely unwell if they develop COVID-19 infection than the general population.
For women who are trying to conceive, or who are in early pregnancy, there is no evidence to suggest an increased risk of miscarriage with COVID-19.
Furthermore, there is also no evidence that the virus can pass to your developing baby while you are pregnant (this is called vertical transmission) or that the virus will cause abnormalities in your baby.
Some babies born to women with symptoms of COVID-19 in China have been born prematurely. It is unclear whether coronavirus was the causative factor, or the doctors made the decision for the baby to be born early because the woman was unwell. Newborn babies and infants do not appear to be at increased risk of complications from the infection.”
RESOURCES
For other resources, here is a list of other links. Many info sites are repetitive. As you are my patients, you are obviously more intelligent, so you don’t need the repetition. (If you are seeing another doctor and are ‘cheating’ by reading I can simplify it or recommend lots of repetition to help get it into your head). I have cherry-picked the most helpful pages (in my opinion).
Our RANZCOG college statement:
https://ranzcog.edu.au/statements-guidelines/covid-19-statement
Statement from the British (Royal College of Obstetricians and Gynaecologists) O&G website (they have been very up to date and informative):
https://www.rcog.org.uk/en/guidelines-research-services/guidelines/coronavirus-pregnancy/covid-19-virus-infection-and-pregnancy/
If you are struggling with the anxiety regarding volde-virus then read this:
https://headtohealth.gov.au/covid-19-support
This information for patients is issued by an excellent (especially for the Yanks… ;-)) American medical app:
https://www.uptodate.com/contents/coronavirus-disease-2019-covid-19-the-basics/print?topicRef=126981&source=see_link
General LOCAL information:
National:
https://www.health.gov.au/news/health-alerts/novel-coronavirus-2019-ncov-health-alert?utm_source=health.gov.au&utm_medium=redirect&utm_campaign=digital_transformation&utm_content=health-topics/novel-coronavirus-2019-ncov
Victorian:
https://www.dhhs.vic.gov.au/coronavirus
WHO Q&As on coronavirus (I have an issue with WHO so I left it until last but this is kind-of good).
https://www.who.int/news-room/q-a-detail/q-a-coronaviruses
Australian National Coronavirus Helpline
Call this line if you are seeking information on coronavirus (COVID-19). The line operates 24 hours a day, seven days a week.
1800 020 080
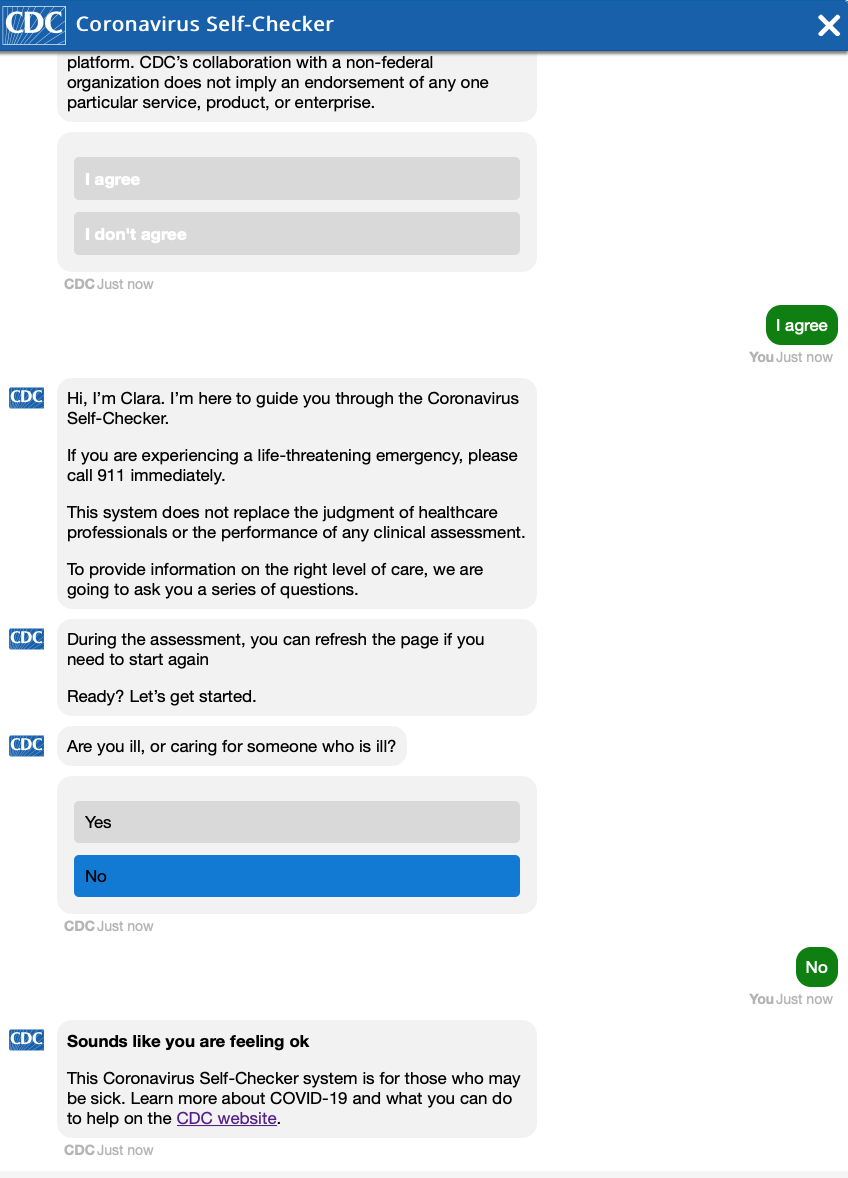
*Interestingly, the CDC has a Coronavirus Self-checker page. I started doing it. See the results in the photo below.
ADVICE
Hang in there people.
I am still working on setting up Instagram (Katie Babs……)
And now I have heard about Facebook live I might do that. (Until I do please get hold of a soft filter for your computer so I look ridiculously young and fresh on video).
RIDICULOUS MUSINGS
The following information is rated MA. It contains horror and adult themes….
*and it is a joke, don’t actually try this at home (that is for the other doctors’ patients. My patients will get it.)
Just in case we go into full lockdown and you are too scared to venture outside your home, I have taken a photo of necessary items to perform home births. I can even Zoom conference you to provide guidance. If you cannot work out what the items are or what they are for, then just add a comment. Happy to take you through it later. Maybe that can be your activity for the day while you are in lockdown…pick the birth kit items.

Option 1

Option 2

Option 3
Update for Current Patients – 25th March (Morning Edition)
Good morning lovely patients. I will try to update as regularly as I can but don’t want to waste your time. My plan is to update you regarding:
– Logistics
– Information
– Resources
– Advice (and general ridiculous musings by myself to you)
LOGISTICS
Today the office is closed. Don’t panic, we are all well.
There are some days I do not consult due to other commitments. Today I am working from home (unless someone decides to have an emergency or let their baby fall out of them). It has been a frantic time for me and I need some time to regroup and strategise. I have scheduled surgery that needs consideration. My public hospital commitments at the Royal Womens require me to make plans with my team there to continue our duties to the general public.
I also need to make a lot of phone calls and attend to usual clinical duties.
I normally staff my office when I am not there, but these times necessitate that I protect my staff – both from unnecessary exposure by coming to work and from Erin and Zoe infecting each other. Hence, from now I will only have one staff member in at a time for 1-2 weeks, then they will swap. Don’t stress about them being unemployed and not getting an income – I have put into place a strategy to keep them being paid and ensure the practice stays open. They are part of my ‘family’ and I want to protect them and their families.
So any non-urgent calls need to wait until tomorrow – including appointments/ scheduling queries.
In the coming weeks my staff will be stretched – I usually need 2 staff to deal with the clinic requirements and attend to my diva-style needs (the regular coffee service on a tray, for example). So with only one staff member they will be a little frazzled (I will try to dial-down the diva behaviour) so BE NICE TO THEM EVEN IF YOU ARE STRESSED.
Anyone booked for tomorrow – please check this page later today for instructions. I will be reviewing every patient’s file to determine if they need to come in or if any special arrangements need to be made – including those booked for GTTs. However, unless otherwise instructed, attend for your usual appointment.
Any urgent calls can be made directly to the birth suite of your hospital (first port of call if you are over 24 weeks gestation) or you can page me on 9387 1000 if you are under 24 weeks or are directed to by the birth suite. This always applies – C-19 or not.
I will remind you all again later but CAESAREAN SECTIONS ARE NOT “ELECTIVE SURGERY” for the purposes of government restrictions. Even ‘elective’ (maternal choice) caesarean sections will proceed. Nobody will make you have a vaginal birth. Babies need to come out REGARDLESS of C19 and the way they come out is the same as if Volde-Virus didn’t exist.
INFORMATION
I will be reviewing any new data and getting back to you with specific instructions about C19 (I can’t bring myself to use its full name – I think it is like the Voldemort of Viruses – I don’t want to speak its name).
RESOURCES
As for information.
ADVICE
Limit your phone surfing, turn off the ABC (unless you are watching ABC for Kids. Peppa Pig is a tonic during these times). Give yourself some C19 free time.
Go for a walk today. Fresh air, exercise is critical to physical and mental well-being. The sky is not falling in, believe it or not. Seeing the beauty of nature reminds us of how beautiful life is. Smile (from a distance) to people you walk past. We all need to signal to our human family that we are connected.
I’ll be back in touch later today.